
Skin Rash Assessment Tool
Check Your Symptoms
Select all symptoms that apply to your current rash. This tool helps identify potential rash types and suggests appropriate next steps.
If you’ve been prescribed Lisinopril‑HCTZ is a combo pill that mixes an ACE inhibitor (lisinopril) with a thiazide diuretic (hydrochlorothiazide) to lower blood pressure. It works well for many, but a frustrating side effect pops up for some users: itchy, red, sometimes painful skin rashes. You’re probably wondering whether you have to ditch the drug, how to soothe the irritation, and what you can do to keep your skin happy while still controlling hypertension.
Quick Takeaways
- Identify the rash early - look for redness, bumps, or swelling that appears after starting or adjusting the dose.
- Start with gentle skin care: fragrance‑free cleansers, moisturizers, and cool compresses.
- Over‑the‑counter antihistamines (e.g., cetirizine) can calm itching, but always check with your doctor.
- If the rash spreads, blisters, or involves mucous membranes, seek medical attention immediately.
- Discuss dose reduction or switching to an alternative antihypertensive if the rash persists.
Why Lisinopril‑HCTZ Can Trigger a Rash
Both components of the combo have skin‑related side‑effect profiles. Lisinopril is an ACE inhibitor that can cause a rare but well‑documented condition called ACE‑inhibitor‑induced angio‑edema, which often starts as facial swelling but may present as a rash. Hydrochlorothiazide, a thiazide diuretic, is notorious for photosensitivity and allergic dermatitis. Together, they raise the odds of a lisinopril rash because the immune system gets two different chemical signals to react to.
Mechanistically, the ACE inhibitor blocks the conversion of angiotensin I to angiotensin II, leading to an increase in bradykinin - a peptide that dilates blood vessels but also inflames skin. Meanwhile, the diuretic can accumulate in skin tissue, especially after sun exposure, acting like a hapten that the immune system flags as foreign. The result? a rash that can range from mild erythema to serious conditions like Stevens‑Johnson syndrome.
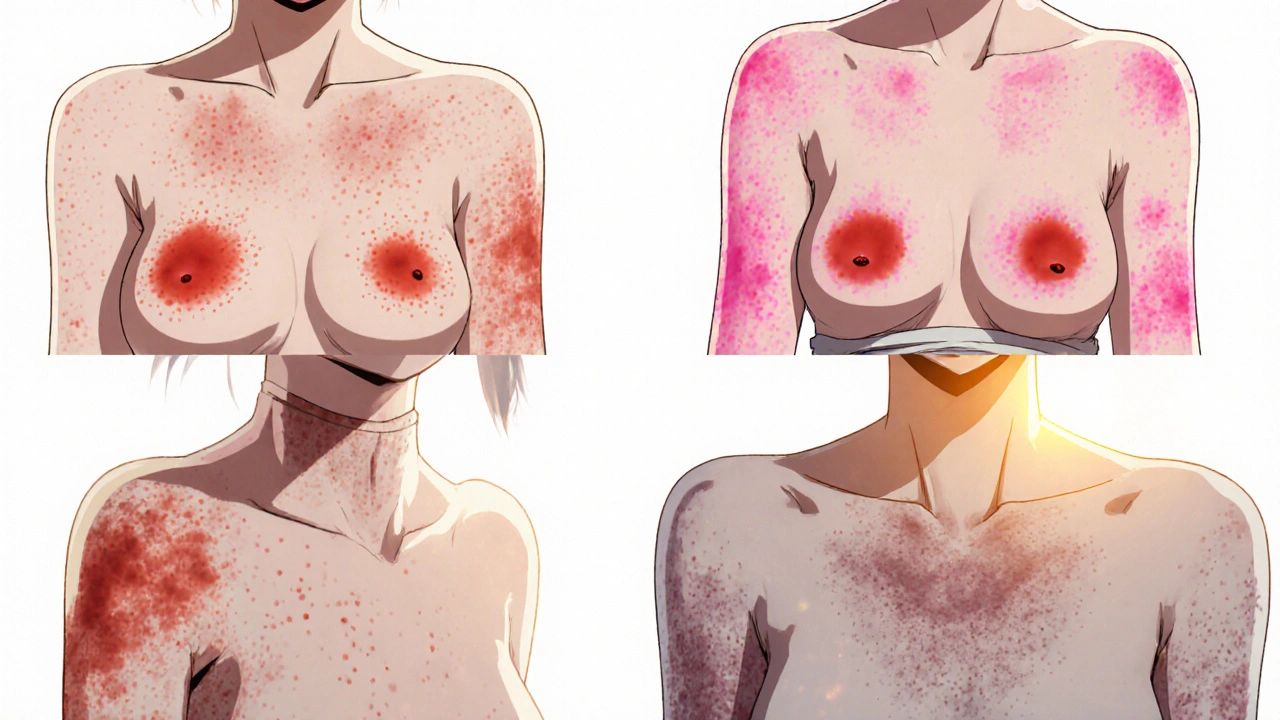
Spotting Different Types of Drug‑Induced Rashes
Not all rashes look the same. Knowing the pattern helps you describe it to your pharmacist or doctor.
- Maculopapular rash: flat red patches with small raised bumps, usually spread over the torso and arms.
- Urticaria (hives): itchy welts that appear suddenly and may move around the body.
- Photosensitivity dermatitis: redness and swelling limited to sun‑exposed areas like the forearms, neck, and face.
- Stevens‑Johnson syndrome (SJS): severe blistering, mucosal involvement, and fever - a medical emergency.
If your rash shows blisters, involves the eyes or mouth, or comes with fever, call emergency services right away. Most rashes from Lisinopril‑HCTZ are milder, but catching the serious ones early saves lives.
Immediate Steps When a Rash Appears
- Stop scratching. Scratching worsens inflammation and can introduce infection.
- Cool the area. Apply a clean, cool compress for 10‑15 minutes, three times a day.
- Switch to a gentle cleanser. Use fragrance‑free, pH‑balanced soap; avoid exfoliants.
- Moisturize. Choose a thick, hypoallergenic ointment (e.g., petrolatum or ceramide‑rich creams). Apply while skin is still damp.
- Take an antihistamine. A daily dose of cetirizine 10mg can reduce itching. Check with a clinician if you’re on other medications.
- Document the rash. Photograph it, note the date it started, dose changes, and any sun exposure. This record helps your doctor decide whether the drug is the culprit.
Long‑Term Skin‑Care Strategies
Beyond the first‑aid steps, a consistent routine keeps skin resilient.
- Barrier repair moisturizers: Look for products with ceramides, hyaluronic acid, and niacinamide. Apply twice daily.
- Sun protection: If hydrochlorothiazide is the trigger, a broad‑spectrum SPF30+ sunscreen (Zinc oxide formulation works well) is essential, even on cloudy days.
- Hydration: Drink at least 2liters of water daily; diuretics increase fluid loss and can dry out the skin.
- Dietary support: Omega‑3 rich foods (salmon, flaxseed) and antioxidants (berries, leafy greens) help modulate inflammation.
- Gentle fabrics: Choose cotton over synthetic blends; avoid tight sleeves that trap sweat.
When to Adjust or Switch Your Medication
Talk to your prescriber if any of these are true:
- The rash doesn’t improve after 7‑10days of skin‑care measures.
- You notice flare‑ups after each dose increase.
- The rash spreads to new body parts.
- Lab tests show eosinophilia (high eosinophil count), signalling a systemic allergic response.
Your doctor may:
- Reduce the dose of Lisinopril‑HCTZ.
- Swap the ACE inhibitor for an ARB (e.g., losartan) that carries a lower angio‑edema risk.
- Replace the thiazide with a potassium‑sparing diuretic (e.g., spironolactone) if photosensitivity is the main issue.
Never stop the medication abruptly; sudden blood‑pressure spikes can be dangerous.
Over‑the‑Counter and Natural Adjuncts
Some people find relief using non‑prescription options, but always discuss them with a pharmacist.
| Ingredient | Typical Onset | Best Use Cases | Pros | Cons |
|---|---|---|---|---|
| Cetirizine cream (1%) | Within 30minutes | Urticaria, mild itching | Fast relief, non‑systemic | May cause local irritation |
| Hydrocortisone 1% ointment | 1‑2hours | Maculopapular rash, inflammation | Proven anti‑inflammatory | Not for prolonged use on large areas |
| Calamine lotion | 15‑30minutes | Cooling effect for mild dermatitis | Readily available, cheap | May dry skin further |
For a natural boost, consider adding Licorice root extract (glycyrrhizin) to your routine. Small studies show it can dampen inflammatory pathways triggered by ACE inhibitors. Again, check dosage because high amounts can affect potassium levels.
Red Flags: When to Seek Emergency Care
A rash is usually manageable, but these signs scream “call 911”:
- Rapid swelling of the face, lips, tongue, or throat.
- Blistering that covers more than 10% of body surface.
- Fever above 38.5°C (101.3°F) with rash.
- Difficulty breathing or wheezing.
These symptoms suggest a severe drug reaction such as SJS or anaphylaxis. Prompt treatment with intravenous antihistamines and steroids can be lifesaving.
Frequently Asked Questions
Can I continue Lisinopril‑HCTZ if I get a mild rash?
Mild rashes often respond to skin‑care measures and antihistamines. Keep a close eye on the rash’s size and intensity. If it doesn’t improve within 10days, schedule a follow‑up to discuss dose adjustment or switching drugs.
Are there specific foods that worsen the rash?
There’s no direct food‑rash link, but high‑sodium meals can increase thiazide‑related dehydration, which may dry skin and amplify irritation. Stick to a low‑salt diet and stay hydrated.
Is it safe to use sunscreen while on Lisinopril‑HCTZ?
Absolutely. In fact, sunscreen is recommended because the thiazide component can cause photosensitivity. Choose a mineral sunscreen with zinc oxide or titanium dioxide to avoid chemical irritants.
What over‑the‑counter antihistamine works best?
Cetirizine 10mg once daily is a popular first‑line choice because it’s non‑sedating and doesn’t interact with most antihypertensives. Loratadine is another option if you’re sensitive to cetirizine.
Could the rash be caused by something else, not my medication?
Yes. New soaps, detergents, or even a recent change in laundry routine can mimic drug‑induced dermatitis. That’s why keeping a symptom diary helps differentiate triggers.
Lauren Sproule
hey everyone if you got that itchy red rash from lisinopril‑hctz try a gentle fragrance‑free cleanser and keep the skin moisturized it can really calm things down
also remember to avoid scratching cuz that just makes it worse